These are mulberry like lesions of varying sizes and thickness resembling “pools or lakes of blood”. They can occur in any part of the central nervous system but are usually located in the upper regions of the brain called the cerebrum. Some cavernous malformations can occur in families as part of a syndrome. Special sequences of MRI like the GRE sequences are best to identify brain cavernous malformations. The incidence ranges from ranges from 0.4% to 0.8% in the general population. The risk of rupture of a cavernoma located in the cerebrum is around 0.5% per year, while the risk of rupture of infratentorial (brainstem and cerebellar) cavernoma is 3.5%. The 3 methods of treatment are srugery, radiosurgery and conservative management.
Brain stem cavernous malformation with bleed
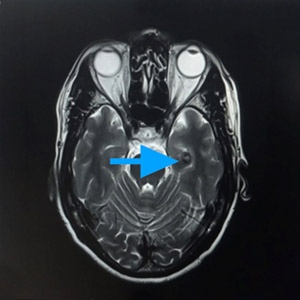
Another brainstem cavernous malformation
Cavernous malformations in various locations in the brain
Arteriovenous malformations (AVMs)
Arteriovenous malformations are developmental anomalies of the arteriovenous system connecting the arteries directly to the brain venous system without any intervening smaller sized vessels in between.
Incidence:The annual new detection rate incidence of AVMs is approximately 1 per 1,00,000 a year. The prevalence in adults is approximately 18 per 100,000
Presentation: Many of the AVMs remain asymptomatic. They can present with a bleed, seizure, headache, gradual reduction in the brain function or cognition.
Rate of bleed: The risk of bleed of an AVM is approximately 4% per year
MRI image of a brain arteriovenous malformation
Image of a surgery for AVM after endovascular embolization to reduce the blood supply to the AVM.
Management: Management of the AVM depends on its mode of presentation, location and size. Many unruptured AVM are now treated conservatively per the ARUBA trial findings. However, one has to weigh the risk of bleed with conservative treatment based on the AVM morphology.
Surgery for AVM: It involves removal of the AV malformation from its location in the brain. Surgery is now performed after endovascular embolisation procedure to reduce the size and blood flow to the AVM. This reduces the chance of bleed during surgery and makes surgery safer.
Endovascular embolisation: This involves sealing the blood supply to the AVM by special agents like bioglue or Onyx, SQUID embolic material. This is done following a digital subtraction angiogram to study the AVM and blood vessel architecture. Then small catheters (microcatheters) close to the blood vessel feeding the AVM and the AVM structure is sealed (Embolised). This gradually shuts off blood supply to the AVM and reduces flow across it.
Radiosurgery for AVM: It involves delivery of a focused dose of radiation to the AVM in a single sitting. The dose is planned by a radiation specialist. It takes upto 1.5 years for the gamma knife ( stereotactic radio surgery) to act and show results.

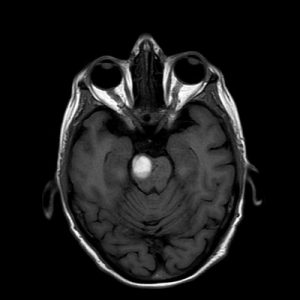 Brain stem cavernous malformation with bleed
Brain stem cavernous malformation with bleed
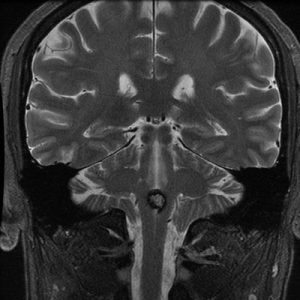 Another brainstem cavernous malformation
Another brainstem cavernous malformation


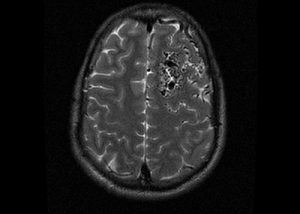 MRI image of a brain arteriovenous malformation
MRI image of a brain arteriovenous malformation
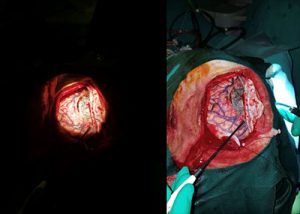 Image of a surgery for AVM after endovascular embolization to reduce the blood supply to the AVM.
Image of a surgery for AVM after endovascular embolization to reduce the blood supply to the AVM.
